Idiopathic low back pain
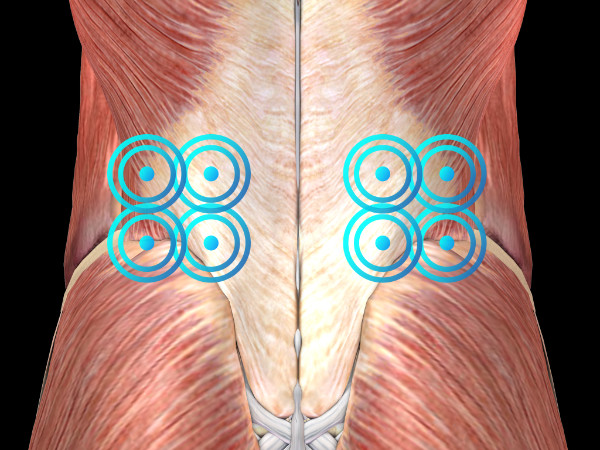
RADIAL PROTOCOL
Radial protocol values
Pressure: 2.5 bar
Pulses: 5,000
Frequency: 12 Hz
Applicator: 15 mm trigger
Total energy flux density dose: 318 mJ/mm²
Number of sessions: 3 (1 per week)




Medical Information
Low back pain without sciatica, stenosis, or severe spinal deformity (hereinafter referred to as idiopathic low back pain (ILBP)) is common and affects people of all ages. It is the second most common condition after the common cold and one of the leading reasons for visits to medical practices.
Its point prevalence reaches 33%, its annual prevalence 73%, and its lifetime prevalence exceeds 70% in most industrialized countries, with an annual incidence ranging from 15% to 20% in the United States. Among physically active adults who do not seek medical care, the annual incidence of clinically significant idiopathic low back pain associated with functional disability is approximately 10% to 15%.
Over recent years, an alarming increase in the prevalence of chronic idiopathic low back pain has been observed in industrialized countries, affecting both men and women of all ages and ethnic backgrounds.
The social and economic impact of ILBP is highly significant. It is the leading cause of disability in individuals under 45 years of age. In its acute form, it typically lasts between three and six weeks before resolving, although relapses are common and low-intensity symptoms often reappear years after the initial episode.
Risk factors for developing disabling ILBP, whether chronic or persistent (i.e., lasting more than three or six months), include prior psychological distress, the presence of compensation-related conflicts, other forms of chronic pain, and job dissatisfaction. Diagnosis is based on clinical characteristics. Imaging studies should be used to rule out other causes of low back pain (particularly in chronic cases) or to confirm the diagnosis of ILBP when uncertainty exists.
The treatment goals for patients with ILBP are:
To relieve pain, restore mobility, accelerate recovery so the patient can return to normal daily activities as soon as possible, prevent the development of chronic conditions, and restore the patient’s physical and economic independence, while maintaining long-term comfort and functionality.
However, the treatment of patients with ILBP presents several challenges:
Most cases of back pain have no identifiable cause; underlying systemic disease is uncommon; most episodes of back pain are unavoidable; and, most importantly, few treatments, if any, have demonstrated clear effectiveness for ILBP.
These treatments include bed rest, exercise, nonsteroidal anti-inflammatory drugs (NSAIDs) and paracetamol, muscle relaxants and opioids (when paracetamol or NSAIDs fail to relieve pain), physiotherapy, and ultimately surgery (in cases of cauda equina syndrome, infections, tumors and fractures compressing the spinal cord, mechanical spinal instability, and possibly intractable pain with a positive Lasègue sign that does not respond to conservative therapeutic measures).
However, the analgesic effects of many treatments for non-specific low back pain are modest and do not differ significantly between acute and chronic patient populations. Radial extracorporeal shock wave therapy (rESWT®) represents an alternative to conservative treatments and should be considered before surgical intervention is proposed.
STUDIES
Bauermeister W.
Stosswellentherapie beim idiopathischen Rückenschmerz pseudoradikulären Syndromen. In: Maier m, Gillesberger F: Abstract 2003 zur Muskuloskelettalen Stosswellentherapie: Norderstedt, 2003, 29-34. Refer to the study.